


Cognitive Therapy for Emetophobia
Cognitive therapy for emetophobia is a protocol designed to treat emetophobia without the use of ERP but still work within the evidence base of CBT.
It draws on influences from:
Cognitive therapy for panic disorder - Clark & Salkovskis
Cognitive therapy for social anxiety disorder - Clark (2001)
Cognitive therapy for illness anxiety disorder- Salkovskis, Warwick & Deale (2003)
Cognitive therapy for OCD - Salkovsiks (2007)
Cognitive therapy for PTSD - Ehlers & Clark (2000)
CBT for Emetophobia – David Veale (2009)
Cognitive therapy for Emetophobia, is built on the cognitive rationale that Emetophobia is caused by inaccurate appraisals about vomiting, nausea, anxiety and uncertainty. These appraisals are being maintained by the excessive use of safety behaviours and avoidance.
Treatment involves:
Idiosyncratic cognitive formulation.
Theory A and B.
Behavioural experiments to remove maintenance processes.
Acceptance of thoughts, feelings as opposed to control.
The theoretical paper can be read below or click here to read a step a step-by-step breakdown of how to apply it to treatment.
Cognitive Therapy for Emetophobia (in press) - David Kaneria
Abstract:
This article proposes a cognitive model for the understanding of Emetophobia, its maintenance and treatment. Emetophobia (the fear of vomiting) is often conceptualised through conditioning or trauma‑fusion models. While these treatments have been shown to be effective, there is a lack of choice for patients regarding treatment, meaning that if treatment has been unsuccessful, clients are often forced to look for less evidence based strategies for which the internet is happy to provide. This leads to considerable frustration, financial cost and the prolonging of distress of those suffering from emetophobia. Current models mainly focus on the use of exposure and response prevention (ERP) which is rooted in behavioural therapy and doesn’t focus on the cognitive mechanisms behind the disorder. This article proposes a cognitive model for emetophobia which is hoped to provide an alternative treatment for when ERP therapy has not been effective or when clients struggle to engage. The clinical implications of this is that cognitive therapy may be more acceptable than ERP‑heavy protocols which can sometimes suffer with client drop out and can feel intimidating for patients to engage in.
Introduction
The specific phobia of vomiting (also known as emetophobia) is a greatly debilitating phobia which can affect every area of the sufferer's life. Unlike most specific phobias, where the sufferer can easily avoid their phobic object, those with emetophobia are fearful of internal sensations and a reflex action (vomiting) which is outside of their control or ability to avoid. The prevalence of emetophobia has been estimated to be up to 8.8% of the population (van Hout & Bouman, 2011). Despite this high prevalence rate, Emetophobia remains an under-researched disorder (Veale & Lambrou, 2006)
The most used treatment protocol for Emetophobia is CBT. This is usually split between behavioural based therapies using exposure and response prevention (ERP) (Craske et al., 2006) or the Veale protocol (Veale, 2009) which is based on the theory that past aversive memories of vomiting become associated with fear and the development and maintenance of emetophobia. One potential issue of basing treatment on traumatic past memories of vomiting is that some patients with Emetophobia fail to report or remember a distinct early memory of vomiting. A small proportion of the population also report not experiencing mental imagery, known as Aphantasia. To the authors knowledge there has been no research into whether or not those with Aphantasia are immune or still experience emetophobia.
The problem with exposure based therapies is that whilst patients often understand the rationale and are satisfied with the treatment (Cox et al., 1994), it often has a PR problem (Richard & Gloster, 2007) and some patients find the idea of exposure therapy distressing (Lipsitz et al., 2001). There has recently been a rise in anti exposure based therapies in the online community which has been enhanced and promoted by the use of social media by groups offering non-exposure based therapies for emetophobia. These groups strongly promote the message that exposure therapies do not work for emetophobia and many emetophobic clients have heard and repeat these messages in online groups. This can lead to the avoidance of treatment. When exposure based interventions are used, some patients struggle to habituate to their anxiety (Pence et al., 2010) or that exposure to situations linked to vomiting is hard to achieve. Exposure therapy is also slower to treat the emotions of disgust (Ludvik et al., 2015) which can be highly prevalent in emetophobia.
This article aims to introduce the idea that Emetophobia can also be understood as a disorder of cognition linked to perception rather than a disorder of conditioning or trauma memories. This approach is called Cognitive Therapy for Emetophobia.
Cognitive Therapy Treatment Protocol:
Treatment aims:
Cognitive therapy for emetophobia takes the view that the patients’ appraisals around vomiting are inaccurate and need to be reappraised. This often clusters in 4 main areas.
· Severity: Appraisals of vomiting being severe or catastrophic need to be reappraised to the idea that although vomiting is unpleasant, it is not catastrophic.
· Likelihood: Appraisals that vomiting is highly likely needs to be appraised to the idea that vomiting is a rare occurrence.
· Coping: Appraisals of the inability to cope with vomiting or anxiety need to be reappraised to the idea they can learn to cope through vomiting and anxiety.
· Control: Appraisals over the need or necessity to have control over vomiting needs to be appraised that control over vomiting is the problem and that instead they should surrender control and instead start living their life.
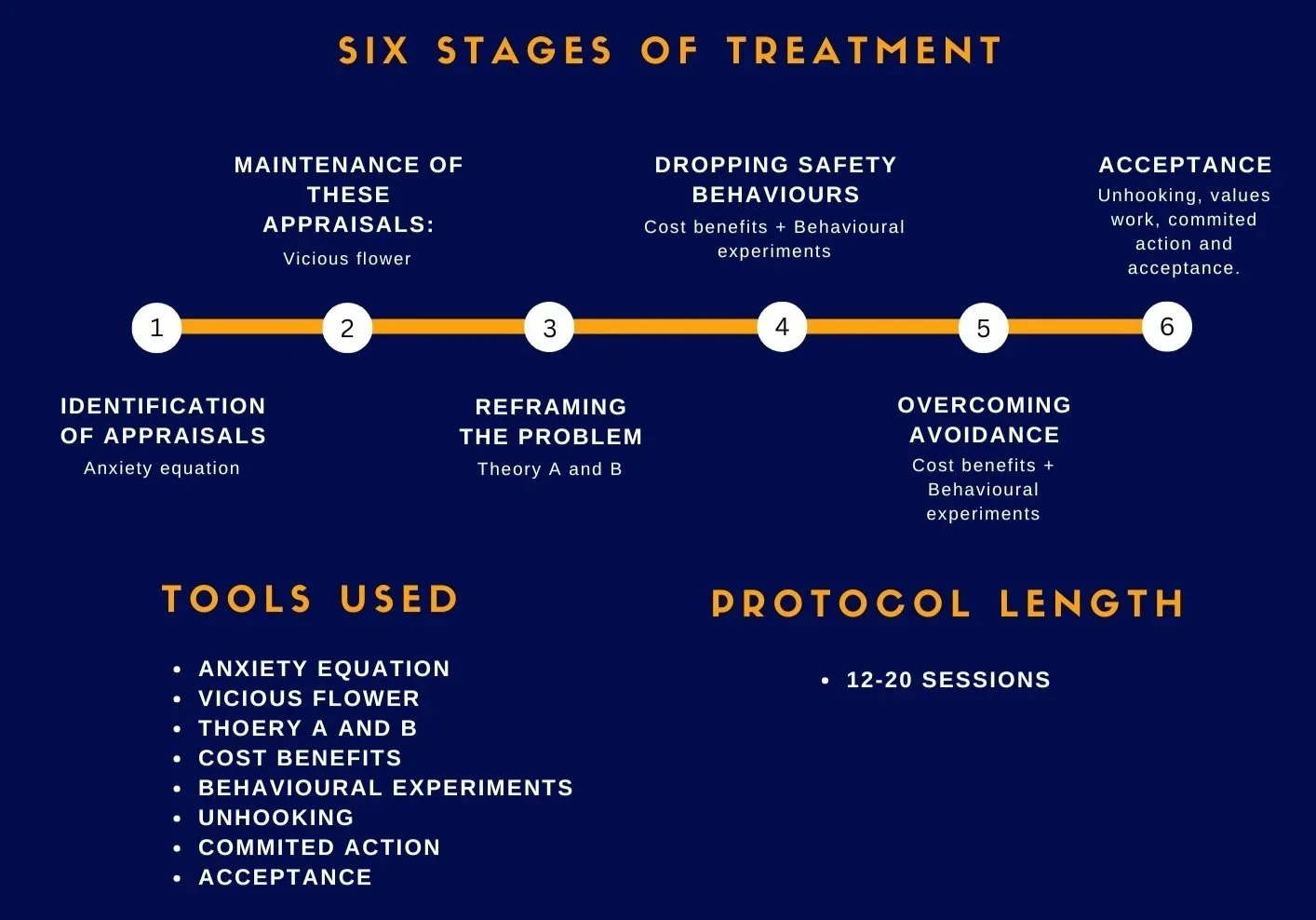
Cognitive therapy for emetophobia follows a six-stage process to treatment:
Stage 1 - Identification of appraisals - Anxiety equation:
As this is a cognitive protocol. The first step is to understand the client’s idiosyncratic appraisal of vomiting. This often extends beyond the act and should also include these areas were relevant:
· The anticipatory anxiety.
· Post vomiting sequalae (The aftermath of vomiting can sometimes be perceived as more psychologically disruptive than the event itself).
· Nausea.
· Uncertainty.
· Anxiety/panic.
· The need for control.
· The likelihood of vomiting to occur.
· Their perceived ability to cope or be supported.
Stage 2 - maintenance of these appraisals – Vicious flower:
The maintenance of the clients’ appraisals should be formulated. This is done by exploring the patients cycle when triggered (thoughts, anxiety, mental imagery and physical sensations) and by exploring the safety behaviours. Formulation is best done using a multi layered vicious flower as outlined later in the article.
Stage 3 - Reframing the problem – Theory A and B:
Those with emetophobia view vomiting as the problem. Cognitive therapy aims to reframe this as the client’s interpretation and reaction (safety behaviours) to vomiting is the real problem. The client can be introduced to this idea using a tool called Theory A and B.
Stage 4 - Dropping safety behaviours – Cost benefits + Behavioural experiments:
The aim of cognitive therapy is to help the client reappraise vomiting as less catastrophic. These appraisals are resistant to direct reappraisal using methods like cognitive restructuring or due to the natural exposure to vomiting when sick due to the patient’s use of safety behaviours preventing disconfirmation. Much of this protocol involves reducing safety behaviours.
This is done in a structured way for each behaviour:
1) Target a behaviour: Pick a type of safety behaviour to work on. Leaving avoidance to last.
2) Define: Define the behaviour. Explore the specifics. What, when, where, with who.
3) Identify beliefs of helpfulness: Explore why the patient is doing the behaviours and what they are trying to achieve. These beliefs changes based on the type of safety behaviour but usually involves one or more of these ideas:
· It helps them monitor and spot danger.
· It helps them be more prepared if vomiting was to occur.
· It prevents vomiting.
· It reduces their anxiety.
4) Discuss the costs: Discuss the costs of the behaviour that identified from the vicious flower and expand on them. Step 3-4 should be done in a table format to make costs benefit analysis.
5) Behavioural experiment: An experiment should be created to test the clients’ beliefs that their safety behaviour is helpful. Usually this requires out of session work.
6) Reflect on the outcome: Learning should focus on if the safety behaviour is helpful, needed, or if the costs of using it are too high. This allows for a cost benefit of if a safety behaviour is worth it. Learning should be linked back to theory A and B to slowly reappraise the problem away from vomiting and towards interpretation and the use of safety behaviours.
Stage 5 – Overcoming avoidance: Cost benefits + Behavioural experiments:
Avoidance should be worked on using behavioural experiments to test the need for avoidance to be used in the first place. Clients fears rarely occur and if they did, learning can focus on reappraising the severity of vomiting and on increasing coping ability.
Stage 6 – Acceptance: Unhooking, committed action and acceptance:
The last stage of therapy aims to help the client reappraise their need for control over vomiting as their need for control (safety behaviours) is directing impacting their quality of life. Acceptance, unhooking and committed action is introduced as an alternative to control.
The Cognitive Model of Emetophobia
The cognitive model proposed is made up of conceptualising emetophobia in three main “layers” and uses a vicious flower formulation as a basis for treatment.
Layer 1 is the core of the patient’s problem and reflects the patient's inflexible and catastrophic “global negative perception” of vomiting, nausea, anxiety, and uncertainty.
Layer 2 is the patient's vicious cycle in response to triggers. Repeated activation of this layer feeds the patients “global negative perception” of vomiting, nausea, anxiety, and uncertainty.
Layer 3 is the behavioural maintenance processes which directly influence and maintain the previous two layers.
Layer 1: The patients “global negative perception” of vomiting:
The first layer of the conceptualization is labelled as the patient’s “global negative perception” perception of vomiting and explores the patients appraisals as vomiting as well as nausea, anxiety, uncertainty and the need for control. This global perception is best visualised using a tool called the anxiety equation which is often used for other cognitive models such as for OCD (Salkovskis, 1985) or Illness anxiety (Salkovskis et al., 2003).
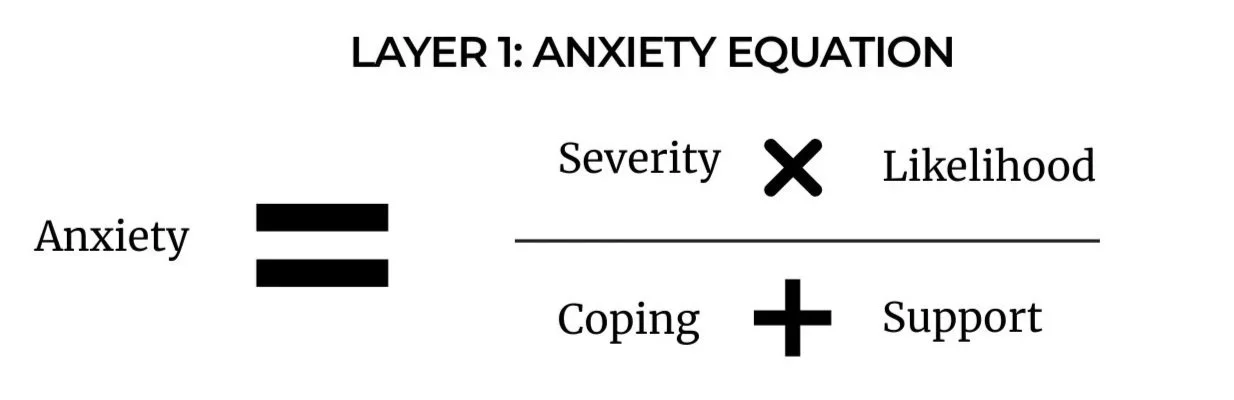
This equation will be idiosyncratic to each patient but usually shows that the patient has over inflated the severity and likelihood and minimised their own ability to cope and be supported (also known as rescue).
Severity:
Those with Emetophobia often have highly catastrophic perceptions of vomiting, nausea, having a high level of anxiety or feeling a lack of control. Patients can fear the physical sensations of nausea, tightness in the throat or other anxiety symptoms (Craske, Barlow and Antony, 2006) and perceive them as dangerous, unacceptable or intolerable. The act of vomiting itself can be appraised as awful, dangerous or disgusting which heightens its perceived severity. Often vomiting is imagined to be truly awful, prolonged, frequent, uncertain and should be avoided at all costs. Often appraisals around vomiting can focus on social judgment or stigma regarding vomiting in public. Some patients believe vomiting is dangerous, lasts forever, or can even lead to death. It is not uncommon for patients to view vomiting as 100% awful and even prefer death to vomiting (Veale, 2009).
If appropriate to the patient, the appraisals of the perceived severity of nausea, anxiety, uncertainty and the need for control can also be incorporated into the equation. Nausea is often seen as a warning or precursor of vomiting, or be seen as intolerable, uncontrollable and that it may last for hours in its own right. Appraisals linked to anxiety can be very important as many patients have distress tolerance and experiential avoidance around feeling anxious or panicked. A minority of emetophobics can perceive the feeling of anxiety when vomiting as worse than the action of vomiting itself. They often believe if they were to vomit, they will panic, shake, be out of control or unable to handle their extreme level of anxiety. Patients may also have appraisals about uncertainty and control. This is similar to appraisals seen in the Intolerance of Uncertainty Model (Robichaud et al., 2019) for Generalised Anxiety Disorder (GAD).
Likelihood:
Those with emetophobia often overinflate how likely vomiting and each specific prediction made in their severity section is to occur.
Coping:
Patients with emetophobia often have a reduced perception in their ability to cope with vomiting, nausea, anxiety or uncertainty. Often this is due to the heightened catastrophic appraisals from their severity section. The more severe the predicted outcome, the harder it is to visualise effective coping. It is not uncommon for those with emetophobia to feel like vomiting is “the end of the world” due to not having any self-confidence in their ability to tolerate or get through the experience.
Support:
The last part of the anxiety equation relates to how patients perceive the support others can or cannot provide if their fears were to occur. In cases where the patient's fear revolves around social judgment or others, support from others is the last thing they want. In some cases patients can perceive a high level of support from others, usually if friends and family members regularly engage in accommodation of safety behaviours.
Conclusion:
This anxiety equation helps form the basis of understanding the patient's global negative perception of vomiting and is the first layer in the cognitive formulation of emetophobia. Treatment revolves around re-appraising these beliefs to a more balanced, less threatening view of vomiting.
Layer 2: The vicious cycle when triggered.
The second layer to the cognitive conceptualisation of emetophobia, represents how the patient responds emotionally, physically and cognitively to a triggering situation. Due to the patient's global negative perception of vomiting, when a patient with emetophobia faces a trigger, it will kickstart a chain reaction similar to this:
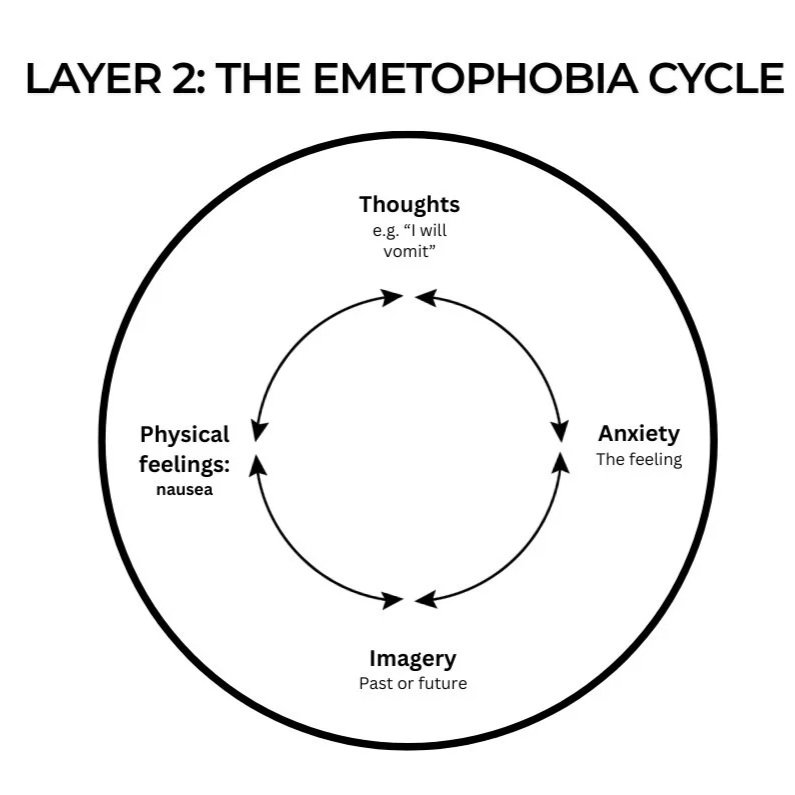
Each patient will have their own different idiosyncratic experience and this should be reflected in their own formulation. However, usually four areas occur:
1) Thoughts: In response to the trigger, the patient will start to have thoughts that validate that they are under threat.
2) Anxiety: Due to these thoughts, the patient's fight and flight system responds to the perceived threat and they naturally feel anxious. This anxiety can feedback into producing more anxious thoughts.
3) Mental Imagery: When the fight or flight response activates, the body naturally orientates itself towards the perceived threat. Due to Emetophobia being an internal and future based threat, the mind often produces a mental picture of vomiting to better visualise and comprehend the threat. This can either be a memory of a past traumatic incident of vomiting or can be a picture of what they fear is about to occur. These mental images increase anxiety and act to validate the patient's thoughts about the current ‘threat’ of vomiting. As previously mentioned, there is a small percentage of the population who can't see or struggle to see clear images in their mind and may skip this step.
4) Physical sensations (i.e nausea and gastrointestinal symptoms): A large majority of those with Emetophobia report experiencing nausea and gastrointestinal symptoms regularly. This can be a direct consequence of this vicious cycle. Mental imagery and thoughts of vomiting or contamination can prompt the defensive emotion of disgust and result in the feeling of nausea. Anxiety (due to the fight and flight response) can also cause nausea as a side effect. The presence of gastrointestinal symptoms is often appraised as confirmation of the risk of vomiting and reinforces the patient's anxious thoughts, leading to more anxiety, which perpetuates the cycle. Depending on the patient's idiosyncratic anxiety equation, patients often report other anxiety symptoms for which they personally find distressing in addition to nausea. These symptoms can also be placed in this section.
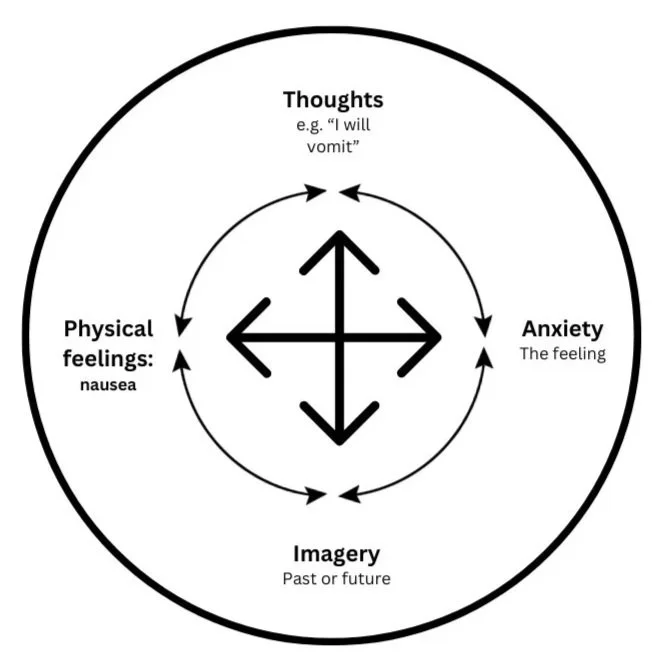
These four components often become a vicious cycle, which over time reinforces the patient's global negative perception of vomiting. This cycle can be represented visually like this:
The arrows on the cycle above do not represent all of the possible interactions between these distinct areas but are designed to show the cyclical nature of this cycle. Layer two could technically be visualised to better show the links similar to this and resemble a four areas model. However, this risks the model looking overly complicated.
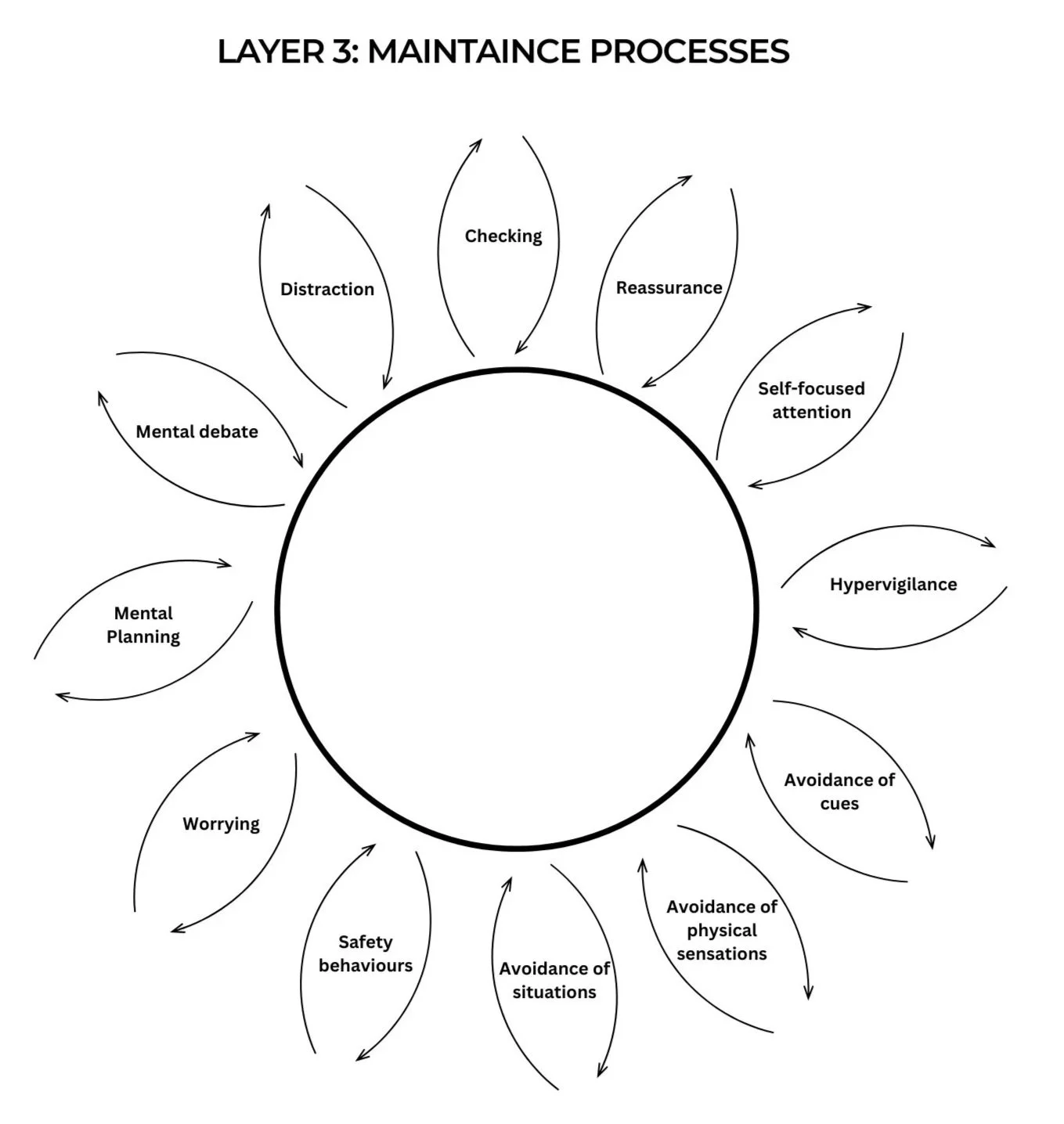
Layer 3: Behavioural Maintenance Processes
The last layer in the cognitive conceptualisation for emetophobia is the maintenance of the first two layers. The maintenance of these layers is hypothesised to be due to the patients excessive use of safety behaviours designed to try and reduce the risk of vomiting. Safety behaviours are any action taken to reduce the chance of vomiting or manage anxiety.
These safety behaviours can be split into various categories:
Actions taken to verify danger and the chance of vomiting:
Checking behaviour.
Reassurance seeking.
Self-focused attention.
Hypervigilance.
Behaviours to avoid or escape vomiting:
Avoiding cues related to vomiting.
Avoiding physical sensations.
Cognitive avoidance.
Avoiding places and situations.
Actions actively taken done to prevent vomiting:
Preventative safety behaviours.
And mental strategies:
Worrying.
Mental planning.
Positive Affirmations/Mental debate.
Distraction.
This is not an exhaustive list and safety behaviours will be idiosyncratic to the patient in question.
Cognitive therapy for emetophobia views these behaviours as a maintaining factor due to:
1) They maintain the global negative view of vomiting in ‘layer one’:
These behaviours unintentionally confirms the patients appraisals in their ‘global negative perception’ that vomiting is catastrophic, highly likely, and something they could not cope with or be supported through.
2) They directly activate and maintain the vicious cycle in “layer two”:
When someone uses these behaviours, they immediately influence what happens in the second layer of the model. This occurs in three ways:
1) Directly cause the four areas in layer 2: Safety behaviours often can directly cause or increase the intensity of thoughts, anxiety, mental imagery or physical symptoms. For example, the behaviour of self-focused attention can increase the likelihood of noticing nausea (which starts the vicious cycle) or amplify its intensity (amplifies the cycle when already activated).
2) Short term relief: Secondly, these behaviours have the ability to stop or reduce thoughts, anxiety, mental imagery or physical symptoms in the short term, leading to a sense of temporary relief. This temporary relief acts to reinforce and validate the original risk of vomiting, causing the behaviour to be repeated for future triggers as it is now appraised as helpful.
3) Increase preoccupation: Lastly, the use of these behaviours increases pre-occupation with vomiting.
3) These behaviours are appraised as helpful, which becomes self reinforcing, thereby maintaining “layer three”:
Each safety behaviour will have appraisals about their helpfulness. As the behaviour feels functional in the moment, it becomes more likely to be repeated, even when it keeps the overall problem going. Treatment involves testing the accuracy of the helpfulness of these behaviours. The helpfulness of safety behaviours is resistant to being naturally re-appraised due to the tendency for their use to prevent disconfirmation of the original feared outcome. This has been well documented in the literature and is often explained using analogies such as ‘the builders apprentice’, ‘elephants on the track’, ‘vampires and garlic’, or ‘dragons and salt’.
Not all patients will engage in each safety behaviour and the appraisals about the helpfulness of each safety behaviour will be idiosyncratic to the patient but often follow the similar theme of preventing vomiting or reducing anxiety.
These unhelpful behaviours can be visualised as feedback loops on a vicious flower:
For each petal of the flower, briefly bullet point a few examples of each behaviour.
For example, reassurance seeking might have:
From mum.
Chat GPT.
Always asking if my food is cooked.
Asking for reassurance on online forums.
And then discuss and briefly bullet point the downsides, costs or how it feeds back into the cycle. Nearly all safety behaviours will activate a least one part, if not all of the previous layer/s. For example, bullet points for reassurance seeking like look like this:
More thoughts, anxiety, nausea and mental images.
Doubt.
Addictive / short term relief.
Makes me believe the reassurance somehow prevented sickness.
Conclusion
Emetophobia has long been conceptualised through the lenses of conditioning, trauma‑fusion, or exposure‑based learning. While these frameworks have contributed valuable clinical tools and are effective, they do not place emphasis on the cognitive mechanisms that explain the maintenance of the disorder. Having another model can be helpful for patients with unidentifiable trauma memories or when habituation is unsuccessful during exposure based therapies. The cognitive model proposed in this article reframes emetophobia as a problem of catastrophic appraisals. By organising emetophobia into three interacting layers; a global negative perception, the vicious cycle, and the behavioural maintenance, this cognitive model offers a coherent explanation for how the fear is caused, triggered and maintained. This model highlights that the core problem is not vomiting itself, but the meaning patients attach to vomiting, nausea, anxiety, and uncertainty. These appraisals drive the physiological and emotional responses that patients misinterpret as evidence of imminent danger, and then motivate a wide range of safety behaviours that inadvertently reinforce and validate the fear in the long term. Although this model is currently untested and empirical research is needed to test this model and compare cognitive therapy with existing CBT and ERP‑based protocols, the theoretical and clinical foundations outlined here are similar to other successful cognitive protocols such as that for Social Anxiety Disorder (Clark, 2001), PTSD (Ehlers & Clark, 2000), Panic Disorder (Clark & Salkovskis, 2009). It is my hope that the cognitive‑therapy approach in this model provides an alternative to ERP. Rather than only relying on exposure and habituation, treatment can focus on collaboratively testing appraisals, reducing the perceived usefulness of safety behaviours, with the aim of changing the patient’s global negative perception of vomiting. This ‘scientific’ approach used in theory A and B is likely to be more acceptable to patients, reduce dropout, and improve engagement compared to exposure based treatment.
References:
Arntz, A., & Weertman, A. (1999). Treatment of childhood memories: theory and practice. Behaviour Research and Therapy, 37(8), 715–740. https://doi.org/10.1016/s0005-7967(98)00173-9
Clark, D. (2001). A cognitive perspective on social phobia. In International handbook of social anxiety: Concepts, research and interventions relating to the self and shyness. John Wiley and Sons.
Clark, D., & Salkovskis, P. (2009). Panic Disorder. https://oxcadatresources.com/wp-content/uploads/2018/06/Cognitive-Therapy-for-Panic-Disorder_IAPT-Manual.pdf
Cox, B. J., Fergus, K. D., & Swinson, R. P. (1994). Patient satisfaction with behavioral treatments for panic disorder with agoraphobia. Journal of Anxiety Disorders, 8(3), 193–206. https://doi.org/10.1016/0887-6185(94)90001-9
Craske, M. G., Antony, M. M., & Barlow, D. H. (2006). Mastering your fears and phobias : therapist guide. Oxford University Press.
Ehlers, A., & Clark, D. M. (2000). A cognitive model of posttraumatic stress disorder. Behaviour Research and Therapy, 38(4), 319–345. https://doi.org/10.1016/s0005-7967(99)00123-0
Lipsitz, J. D., Fyer, A. J., Paterniti, A., & Klein, D. F. (2001). Emetophobia: Preliminary results of an internet survey. Depression and Anxiety, 14(2), 149–152. https://doi.org/10.1002/da.1058
Ludvik, D., Boschen, M. J., & Neumann, D. L. (2015). Effective behavioural strategies for reducing disgust in contamination-related OCD: A review. Clinical Psychology Review, 42, 116–129. https://doi.org/10.1016/j.cpr.2015.07.001
Pence, S. L., Sulkowski, M. L., Jordan, C., & Storch, E. A. (2010). When Exposures Go Wrong: Trouble-Shooting Guidelines for Managing Difficult Scenarios that Arise in Exposure-Based Treatment for Obsessive-Compulsive Disorder. American Journal of Psychotherapy, 64(1), 39–53. https://doi.org/10.1176/appi.psychotherapy.2010.64.1.39
Richard, D. C. S., & Gloster, A. T. (2007). Exposure therapy has a public relations problem. Handbook of Exposure Therapies, 409–425. https://doi.org/10.1016/b978-012587421-2/50019-3
Robichaud, M., Koerner, N., & Dugas, M. J. (2019). Cognitive behavioral treatment for generalized anxiety disorder : from science to practice. Routledge, Taylor & Francis Group.
Salkovskis, P. M. (1985). Obsessional-compulsive problems: A cognitive-behavioural analysis. Behaviour Research and Therapy, 23(5), 571–583. https://doi.org/10.1016/0005-7967(85)90105-6
Salkovskis, P. M., Warwick, H. M. C., & Deale, A. C. (2003). Cognitive‐Behavioral Treatment for Severe and Persistent Health Anxiety (Hypochondriasis). Brief Treatment and Crisis Intervention, 3(3), 353–368. https://doi.org/10.1093/brief-treatment/mhg026
van Hout, W. J. P. J., & Bouman, T. K. (2011). Clinical Features, Prevalence and Psychiatric Complaints in Subjects with Fear of Vomiting. Clinical Psychology & Psychotherapy, 19(6), 531–539. https://doi.org/10.1002/cpp.761
Veale, D. (2009). Cognitive behaviour therapy for a specific phobia of vomiting. The Cognitive Behaviour Therapist, 2(4), 272–288. https://doi.org/10.1017/s1754470x09990080
Veale, D., & Lambrou, C. (2006). The Psychopathology of Vomit Phobia. Behavioural and Cognitive Psychotherapy, 34(2), 139–150. https://doi.org/10.1017/s1352465805002754
How to apply the theory to practice:

Click the above image for a downloadable PowerPoint presentation
There are six key stages for treating a client using cognitive therapy for emetophobia.
Stage 1 - Identification of appraisals - Anxiety equation:
The first stage of therapy should involve understanding the clients’ appraisals about why they find vomiting distressing. This involves showing the client the anxiety equation and discussing each element. This often takes around 30 minutes or more depending on the client. Some clients have great insight into their thoughts, while others will not. Appraisals will be highly idiosyncratic and, in some individuals, will focus more on anxiety, control and anticipation rather than being sick itself.
During the ‘severity’ section of the equation you can create subheading for common themes such as:
· Vomiting itself.
· The build-up.
· The aftereffects.
· Social fears.
· Appraisals of anxiety itself or panic attacks.
· The lack of control or uncertainty.
· Appraisal of nausea.
Whilst doing this, one of the key aims is to help the patient see that their ‘interpretation’ of vomiting is central to their anxiety. Anyone who has the same thoughts as them would be anxious too. Start planting the seed that these thoughts might not be true.
Following the anxiety equation, it is advised to give some psychoeducation about anxiety focusing on:
· The purpose of anxiety (a warning alarm of potential danger).
· How the anxiety system is designed to be flexible and able to learn about new threats. So flexible that it has incorrectly learnt that vomiting is a threat.
· How perception of danger is more important than factual danger.
Then discuss the ways in which our anxiety system learns to be afraid. Following each point, explore if this occurred for the development of the client’s phobia. Using an analogy of a dog phobia works well for this.
· Direct experiences: e.g. Someone who was attacked by a dog can learn to be afraid of dogs. The same is true for a having bad episode of vomiting.
· Indirect experiences: e.g. Seeing someone else attacked by a dog can teach us to be afraid. The same is true for seeing someone else having bad episode of vomiting.
· Being told: We are social animals and can learn from being told. For example, a parent with a dog phobia might pass the fear on by telling their children that dogs are bad. For emetophobia this can include social media and Facebook groups adding to their phobia.
· We can learn by nothing happening (negative reinforcement): Humans can learn by the perception that we just avoided a bad outcome (regardless of how true that was).
Homework:
· Clients should be instructed to reflect on their anxiety equation and start to recognise it in the moment. This can be done in their mind or written down. The aim is for them to start seeing this equation and their thoughts as interpretations rather than facts.
· It is possible to ask the clients to write down their history of being sick or other events they think lead to the development of their phobia based on the learning types explored in the session.
Stage 2 - maintenance of these appraisals – Vicious flower:
The second stage occurs over the next two sessions and involves using a vicious flower to understand the maintenance of the problem.
This vicious flower has three components:
· The centre of the flower.
· The middle of the flower.
· The petals of the flower.
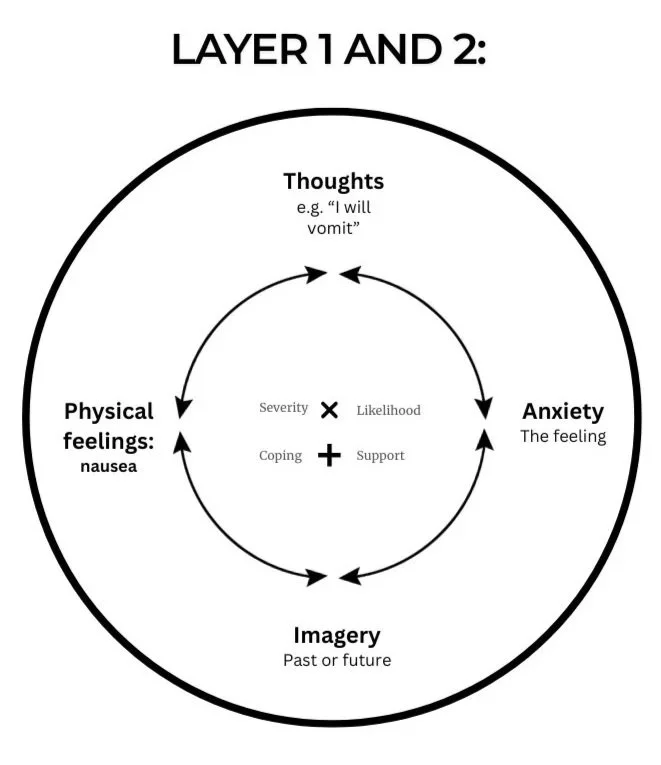
The centre of the flower – Anxiety equation:
This is the anxiety equation. A blank equation can be placed in the centre of the flower to represent this. This equation represents the client’s global negative perception of vomiting which leads to the middle of the flower.
The middle of the flower – Vicious cycle:
The middle of the flower represents how the client reacts when triggered. This is idiosyncratic but often resembles a fours areas model between thoughts, anxiety, mental imagery and physical sensations. This should be quickly explored with the patient and should take no longer than 5-10 minutes. The aim is to help the client see how these four areas are interlinked and that their emetophobia cycle can be started in any of these four areas. Guide the client realise that these four items are directly caused by their negative view of vomiting and how these symptoms only reinforce these appraisals
The petals of the flower – Safety behaviours:
The outside flower is the behavioural maintenance processes. This should be done in the same way as any vicious flower. Briefly define each safety behaviour and explore how it is backfiring. Each behaviour feeds back into one or more of the four components of the previous layer (thoughts, anxiety, mental imagery and physical sensations) and convinces them that their anxiety equation is true.
The aim of this process is to help the client see how their behaviours are only causing their distress and intensifying their negative view around vomiting.
Homework:
Homework following the vicious flower should be for the client to reflect on the costs of using their safety behaviours each time they use them and to monitor if these behaviours are influencing their thoughts.
Stage 3 - Reframing the problem – Theory A and B:
The third stage of therapy takes one session and is designed to help the client reframe the problem away from vomiting and towards the cognitive rationale that it is an interpretation problem. This is facilitated by using a tool called ‘Theory A and B’. This process is the same as in the treatment of panic disorder, illness anxiety disorder or OCD.
Unlike for tother protocols, you can directly provide the client with the two opposing theories and use an analogy to help explain it. I often use a dog analogy of a really friendly dog visited by two people. One person has a dog phobia, and the other person is a dog lover. Ask the client what type of thoughts each person will be having about that same dog. This shows that the dog is not the problem, the interpretation of the dog is. The same might be true for vomiting.
For each theory:
· Explore what evidence supports each theory. Lightly challenge any cognitive biases or distorted evidence.
· How the client should act if each theory is true. Validate that their safety behaviours make total sense and are actually logical actions based upon the assumption that theory A is true.
· Explore the long-term implications for their life of each theory
The aim of this tool is not to convince clients that vomiting is fine. It is to provide a framework to test and facilitate the idea that interpretation of vomiting is the problem and needs to change. Following on from all behavioural experiments and learning in future session, revisit this and see which theory their new evidence supports. The aim is to help prove which theory is true over time.
Homework:
Homework for this session can be to discuss these theories with a trusted person to discuss each theory and explore the evidence in more detail.
Stage 4 - Dropping safety behaviours – Cost benefits + Behavioural experiments:
Stage four is the longest stage in the protocol. The number of sessions differs based on the client’s presentation and need.
Before working on any behaviours, the client needs to be taught a few important things.
1) Why we choose to use a behaviour.
2) How beliefs about the helpful of a behaviour can be maintained by the behaviour itself.
3) How beliefs are testable.
Why we choose to use a behaviour:
In cognitive therapy, the idea is that clients decide to use a behaviour because they think it is the right behaviour to use.
An analogy using can openers can be used to teach this idea.
Follow these steps:
1) Imagine you need to open a can, and you had two can openers. A really good one, and a really bad one. Which one do you choose. Naturally the one that works better.
2) Now imagine you only had one can opener, it isn’t the best. It sometimes works and sometimes doesn’t. Do you still try it? Of course. There is no other option, and it might work so it is worth trying.
3) Imagine you had a completely broken can opener. It is smashed to bits and has no chance of working. You wouldn’t even try it.
4) Imagine your only option was to borrow your friends can opener. It is the best can opener in the world, but he charges you £100 for every use. You wouldn’t use it because it is too expensive.
This shows that we must think a behaviour works or is worth the cost to decide to use it. Whereas if we know it doesn’t work or is not worth the cost we decide to try something else.
How beliefs about the helpful of a behaviour can be maintained by the behaviour itself:
The client needs to be made aware of how safety behaviours can prevent the disconfirmation of thoughts. There are a lot of analogies for this already; dragon-salt, builders apprentice, or elephants on the track. I created one in particular that works well for emetophobia called “barking at the postman” and it goes like this.
Imagine a dog that fears the postman. When the postman comes close to the house, the dog perceives a threat. The dog has a thought that ‘the postman is going to break in’ and so is a danger.
So, the dog barks as aggressively as he can (safety behaviour) and the postman posts his letter and walks off. The dog congratulates himself on getting rid of the threat. He incorrectly learnt that barking keeps the postman away. Good boy! Each day the postman comes and each day the dog barks. Each day his belief that ‘the postman is going to break in’ is validated and his believe that barking is the correct response is also reinforced.
The aim of the story is to help the client see that even though nothing bad happened, the dog could never change his viewpoint because his actions were confirming his belief.
How beliefs are testable:
The client should be introduced to the idea that thoughts are testable predictions and behavioural experiments can be used to test thoughts.
To illustrate this, I usually hold up an object and ask the client “imagine if I had the thought that if I drop this, it will just float in middle air. How could I test how true this thought this?”. Usually, the client says to drop it. Then I drop it, act surprised, laugh and say, ‘I guess that thought was wrong’.
Each session of dropping safety behaviours can follow a similar pattern:
1) Target a behaviour: Pick a type of safety behaviour to work on. Leave avoidance to last.
2) Define: Define the behaviour. Explore the specifics. What, when, where, with who.
3) Identify beliefs of helpfulness: Explore why the patient is doing the behaviours and what they are trying to achieve. These changes based on the type of safety behaviour but usually involves one or more of these ideas:
· It helps them monitor and spot danger.
· It helps them be more prepared if vomiting was to occur.
· It prevents vomiting.
· It reduces their anxiety.
4) Discuss the costs: Discuss the costs identified from the vicious flower and expand on them. Step 3-4 should be done in a table format if possible.
5) Behavioural experiment: Create an experiment to test those beliefs that the behaviour is helpful. Usually this requires out of session work.
6) Reflect on the outcome: Learning should focus on if the safety behaviour is helpful, needed, or if the costs of using it are too high. Link back to theory A and B to slowly reappraise the problem away from vomiting and towards interpretation and the use of safety behaviours.
Homework:
The client’s homework should be to test out the helpfulness and costs of their behaviour. This can be achieved using either:
· Behavioural experiments
· AB/AB experiments
To test, reduce, ban or adjust the frequency or intensity of a safety behaviour. The aim being to show the costs of the behaviour and to demonstrate that the perceived benefits are not likely accurate.
Once they have re-appraise the helpfulness of the behaviour, the client should continue to eliminate the behaviour each week.
Stage 5 – Overcoming avoidance: Cost benefits + Behavioural experiments:
Stage 5 is about overcoming avoidance. Although it is possible to do this before or alongside stage 4, many people with emetophobia really struggle to face their fears in the absence of using safety behaviours. This is why it is often important to build their confidence with dropping these prior to overcoming avoidance.
Overcoming avoidance in cognitive therapy is done using behavioural experiments instead of ERP. The aim is not to try and face everything the client is afraid of or to face unusual situations, it is instead about overcoming avoidance of the things the client SHOULD be facing in their life already on a regular basis. There is often no need for fake throwing up in toilets, vomit flavoured jellybeans or making fake vomit (unless it is clinically needed based on the client’s idiosyncratic formulation).
Start by making a large list of things the client is avoiding. This often clusters around:
1) Physical situations such as places, foods or ill people.
2) Cognitive avoidance to images, thoughts or memories.
3) Avoidance of physical sensations such as avoiding anxiety symptoms or nausea.
4) Avoiding cues and reminders of vomiting such as scrolling past social media videos or hiding from sounds.
This list of avoided things should be added to a behaviour experiment chart. For each avoided situation, explore the feared prediction and why the client believes avoidance is needed. Then for each, discuss how this idea can be put to the test. Then the aim is for the patient to test out if this avoidance is needed by facing these situations (without safety behaviours) one at a time. The goal is to learn if avoidance is needed. This is done on one chart as the learning from each experiment should start telling the same story, that avoidance is not needed. This helps the client to generalise what they have learnt.
The aim of stages 4-5 is to help the client stop trying to ‘prevent sickness at all costs’. Only then can they change how they appraise vomiting. Often many people with emetophobia will tell you they logically know vomiting isn’t dangerous, awful or intolerable. However, I often respond by saying that ‘if you say it is safe, but act like it is dangerous. Who does your anxiety system listen to, your words or actions?’. So, dropping safety behaviors and avoidance is needed for these appraisals to really change. The aim is to help move the client away from acting like theory A is correct and towards acting as if theory B is correct.
If a client was sick during an experiment:
As sickness is an unavoidable part of life, it is possible that clients can be sick during a behavioural experiment. This is often due to random coincidence rather than the experiment. This should always be ruled out and experiments repeated if the client believes they were linked to see how accurate this was.
If the client is ever sick during therapy, focus learning on reappraising its awfulness, likelihood and ability to cope by comparing their experience to their anxiety equation. Often vomiting can be appraised as awful due to emotional reasoning. If the client was highly anxious or panicking, they remember these feelings and it influences how they perceived vomiting. This can be discussed as a learning point.
Stage 6 – Acceptance: Unhooking, committed action and acceptance:
The last stage is designed to help the client reduce their need for control over vomiting. This is achieved by using methods from acceptance and commitment therapy (ACT) to reframe their need for control. This includes:
· Unhooking.
· Committed action.
· Acceptance.
Unhooking:
Clients often take their thoughts and feelings very seriously. Every thought about the potential for vomiting is acted upon as if it was 100% true and every feeling of nausea is appraised as a danger. Clients should be guided towards the idea that their thoughts are just interpretations. Rather than treating thoughts as a fact, it is possible to start recognising thoughts simply as something the mind is generating. Just words and images. This helps the client create distance between themselves and the content of the thought. The aim being to reduces its emotional impact and allow the thought to no longer be a direct signal of danger, but an experience that can be observed and if chosen, not to be acted on.
This is achieved through discussions and asking the client to actively try to unhook from their thoughts. If you are experienced with ACT therapy, you can use any of the various methods for this. If you have little experience of ACT, then simply ask the client to start naming their thoughts as thoughts as they experience them. This creates distance from the content of the thought. Often the phrase “I am having the thought that X” can help. If the client recognises these are just thoughts, and attempts to not act upon it, they can learn how seriously or not these thoughts needed to be acted upon. This pairs up well with dropping safety behaviours.
Committed action:
Once the client is able to recognise that ‘thoughts are just thoughts’. Suddenly they have a choice on how to respond to them. This is were committed action can be used. Again, if you are experienced in ACT, you can use a whole range of your skills here. If you have little or no experience, then committed action can follow these steps:
1) Discussing the difference between goals and values.
2) Discussing the ‘away and towards principal’ – Actions either move us towards or away from our values.
3) Discuss workability – the idea that all actions are specific to the context in which they are used. So, no action is inherently good or bad. The only thing that matters is if they bring you closer or away from your value in any given context.
4) Introduce the idea of a choice point. The client has the ability to choose how to respond to their thoughts, feelings or situations and decide to either make a value-based action or an away move (usually a safety behaviour).
Acceptance:
This last step is designed to help the client realise that they have spent their whole life trying to prevent something that is inherently controllable (illness) and that this need for control is actually a bigger problem than the thing they are trying to prevent. The costs of control and having emetophobia should be explored. This overlaps with the last column done in theory A. The client can be guided to the idea that control never works in the long run. They are ‘paying the costs’ to maintain control and either get the short-term relief or it backfires and starts the emetophobia cycle. Regardless, their fear only grows.
Following this, acceptance should be defined as a behaviour and an alternative to trying to maintain control. Once it is defined as a behaviour, acceptance is now an option to pick at a choice point.
Again, if you are experienced in ACT, you can use a whole range of your skills here around acceptance. If you have little or no experience, then you can use the ‘three A’s of acceptance’.
Acknowledge: Acceptance starts with acknowledging an uncomfortable thought or feeling. Clients should name their experience and try to unhook from it.
Allow: Then they need to be willing to allow that uncomfortable experience. This is about not using safety behaviours or preventing their feeling in anyway.
Accommodate: Once this is done, it is about co-existing with the feeling or thought. Allowing it to stay as long as needed.
This process should be practiced regularly in response to triggers, that way it can also be used when vomiting does occur. When a client accepts vomiting, it helps them reappraise the severity and their ability to cope through it. Often acceptance leads to a reduction in the distress associated with uncomfortable experiences. When used during vomiting, it often makes the episode feel less distressing, which naturally helps reprise the awfulness of it, and increase appraisals of coping.
The aim of stage 6 is to help the client start living their life based on their values and how they want their life to look, not about spending it trying to prevent sickness.